 Overview OverviewUneven muscle tension results in the distortion of one or several of the small toes. (Hammertoes) Pressure points develop at the raised middle joint as well as at the tip of the toe and underneath the metatarsal head. In the beginning, when the misalignment can still be corrected, it often suffices to lengthen the tendon and to cut a notch into the capsule. In a contracted misalignment, part of the middle joint is removed to form a replacement joint. Modern surgical techniques preserve the metatarsophalangeal joint (Weil or Helal osteotomies). Causes As described above, the main reason people develop hammertoes is improper footwear, or footwear that is too short for the toes. Shoes that do not allow our toes to lie flat are the biggest cause of hammertoes, though there are others, including genetics, injury or trauma in which the toe is jammed or broken. Diseases that affect the nerves and muscles, such as arthritis. Abnormal foot mechanics due to nerve or muscle damage, causing an imbalance of the flexor and extensor tendons of the toe. Systematic diseases such as arthritis can also lead to problems such as hammertoe. Some people are born with hammertoes, while others are more prone to developing the condition due to genetics. If you have ever broken a toe, you know there is not much that can be done for it. It is one of the only bones in the body that heals without the use of a cast. A broken toe may be splinted, however, which may help prevent a hammertoe from forming.  Symptoms A hammertoe causes you discomfort when you walk. It can also cause you pain when trying to stretch or move the affected toe or those around it. Hammertoe symptoms may be mild or severe. Mild Symptoms, a toe that is bent downward, corns or calluses. Severe Symptoms, difficulty walking, the inability to flex your foot or wiggle your toes, claw-like toes. See your doctor or podiatrist right away if you develop any of these symptoms. Diagnosis Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe. Non Surgical Treatment In the early stages, the deformities from mallet toe, claw toe and hammertoe can be corrected. But if treatment is delayed too long, permanent stiffness can ensue which can only be corrected by surgery. The most effective treatment options are good fitting footwear. Shoes with a wide toebox will be more comfortable and will reduce the tension on the muscles and friction on the toes. Avoid high heels as they push your feet forwards to the front of the shoes. This increases the pressure on the toes, forcing them to bend more than usual. Shoes should ideally be half an inch longer than your longest toe. Exercises to strengthen and stretch the muscles can be really helpful. Simple things like trying to pick marbles up with your feet or scrunching up a towel underneath your foot can work well. Surgical Treatment In some cases, usually when the hammertoe has become more rigid and painful, or when an open sore has developed, surgery is needed. Often patients with hammertoe have bunions or other foot deformities corrected at the same time. In selecting the procedure or combination of procedures for your particular case, the foot and ankle surgeon will take into consideration the extent of your deformity, the number of toes involved, your age, your activity level, and other factors. The length of the recovery period will vary, depending on the procedure or procedures performed.  Prevention Skin creams can help maintain skin softness and pliability. A pumice stone or loofah sponge can help get rid of dead skin. Taking a warm footbath for 10 minutes two or three times a week will keep the feet relaxed and help prevent mild foot pain caused by fatigue. Adding 1/2 cup of Epsom salts increases circulation and adds other benefits. Taking footbaths only when the feet are painful is not as helpful. Overview
Pronation is the normal movement the foot makes to absorb the impact from walking or running. It occurs once the heel strikes the ground and the foot disperses the impact, stretching and flattening the arch as the foot rolls inward. Supination is the opposite motion of pronation. The foot supinates, or rolls on its outer edge, to help with stability as we walk or run. A reasonable amount of pronation is necessary for the foot to function properly. However, when the foot arch remains flat and the foot rolls inward too much one may have excessive pronation or overpronation. This medical condition can result from continually straining the feet and wearing footwear that lacks sufficient foot arch support.  Causes Generally fallen arches are a condition inherited from one or both parents. In addition, age, obesity, and pregnancy cause our arches to collapse. Being in a job that requires long hours of standing and/or walking (e.g. teaching, retail, hospitality, building etc) contributes to this condition, especially when standing on hard surfaces like concrete floors. Last, but not least unsupportive footwear makes our feet roll in more than they should. Symptoms Eventually, over-pronation can lead to a full list of maladies including flat feet, plantar fasciitis, plantar fibroma, neuromas, heel spurs, shin splints, ankle sprains, bunions, hammertoes, calluses, and pain in the arches, knee, hip and lower back. But it doesn?t have to go that far, because there are steps we can take to correct the over-pronation. In the vast majority of cases, we?ll prescribe custom foot orthotics, which will realign your ankles, redistribute the weight, support the arch and reduce the twisting. Many orthotics will fit snugly into your normal shoes. Although we?ll also take a look at the type of shoes you wear to see if they are contributing to the problem. Diagnosis Your healthcare provider will ask about your symptoms, medical history, and activities and examine your feet. Your provider may watch you walk or run. Check the motion of your feet when they strike the ground. Look at your athletic shoes to see if they show an abnormal pattern of wear.  Non Surgical Treatment Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. These orthotics should be designed with appropriate arch support and medial rearfoot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improperly fitting footwear can lead to additional foot problems. Prevention Massage and stretch the calves to increase dorsiflexion at the foot/ankle. Dorsiflexion is the bending at the ankle. By improving the dorsiflexion, one will have more flexibility at the ankle, which will allow the foot to over-pronate less. Massage the IT Band with a foam roller or tennis ball to quiet down the tightness throughout this part of the leg. The IT Band attaches from the glute maximus and runs down the side of the leg into the knee area. When the IT Band is tight it will accelerate the force of the leg moving inward, which will cause the foot to move inward as well. It is often that tightness through the IT Band that promotes over-pronation. Decreasing over-pronation, which is very prominent in runners, will help add endurance, speed and efficiency to your run and ultimately place less stress on your body.
Overview
 A bunion is a ?bump? on the joint at the base of the big toe-the metatarsophalangeal (MTP) joint-that forms when the bone or tissue at the big toe joint moves out of place. The toe is forced to bend toward the others, causing an often painful lump of bone on the foot. Because this joint carries a lot of the body's weight while walking, bunions can cause extreme pain if left untreated. The MTP joint itself may become stiff and sore, making even the wearing of shoes difficult or impossible. A bunion-from the Latin "bunio," meaning enlargement, can also occur on the outside of the foot along the little toe, where it is called a "bunionette" or "tailor's bunion". A bunion is a ?bump? on the joint at the base of the big toe-the metatarsophalangeal (MTP) joint-that forms when the bone or tissue at the big toe joint moves out of place. The toe is forced to bend toward the others, causing an often painful lump of bone on the foot. Because this joint carries a lot of the body's weight while walking, bunions can cause extreme pain if left untreated. The MTP joint itself may become stiff and sore, making even the wearing of shoes difficult or impossible. A bunion-from the Latin "bunio," meaning enlargement, can also occur on the outside of the foot along the little toe, where it is called a "bunionette" or "tailor's bunion".Causes People born with abnormal bones (congenital) in their feet. Inherited foot type. Foot injuries. Inflammatory or degenerative arthritis causing the protective cartilage that covers your big toe joint to deteriorate. Wearing high heels forces your toes into the front of your shoes, often crowding your toes. Wearing shoes that are too tight, too narrow or too pointed are more susceptible to bunions. Pain from arthritis may change the way you walk, making you more susceptible to bunions. Occupation that puts extra stress on your feet or job that requires you to wear ill-fitting shoes. The tendency to develop bunions may be present because of an inherited structural foot defect. Symptoms Symptoms often include pain, swelling, and abnormal position of the first toe. The technical term for bunions is ?hallux valgus? (HV). This refers to the first toe or hallux moving away or abducting from the middle of the foot and then twisting in such a way that the inside edge actually touches the ground and the outside edge turns upward. This term describes the deviation of the toe toward the outside part of the foot. If left untreated, bunions can worsen over time and cause considerable difficulty in walking, discomfort, and skin problems such as corns. In some cases, a small bursa (fluid-filled sac) near the joint becomes inflamed. This condition is known as bursitis and can cause additional redness, swelling, and pain. Less frequently, bunions occur at the base of the fifth toe. When this occurs, it is called a ?tailor?s bunion? or bunionette. Diagnosis The doctor considers a bunion as a possible diagnosis when noting the symptoms described above. The anatomy of the foot, including joint and foot function, is assessed during the examination. Radiographs (X-ray films) of the foot can be helpful to determine the integrity of the joints of the foot and to screen for underlying conditions, such as arthritis or gout. X-ray films are an excellent method of calculating the alignment of the toes when taken in a standing position. Non Surgical Treatment Changing your footwear to roomy and comfortable shoes that provide plenty of space for your toes. Padding and taping applied by chiropodist/podiatrist to your foot can reduce stress on the bunion and alleviate your pain. Oral medications such as acetaminophen (Tylenol), ibuprofen (Advil, Motrin) or naproxen (Aleve) may help control the pain of a bunion. Cortisone injections. Over-the-counter arch supports can help distribute pressure evenly when you move your feet, reducing your symptoms and preventing your bunion from getting worse. Prescription foot orthotic devices to help stabilize the forefoot. Manual foot therapy to free up motion in arthritic foot joints.  Surgical Treatment The main goal of surgery is to realign the big toe joint in order to relieve symptoms, correct deformity and restore function. Surgery to remove a bunion is known as a bunionectomy. There are many variations of this operation and the type of surgery performed will vary depending on factors such as the degree of deformity, the strength of the bones, the person's age and the surgeon?s preferred approach. Most surgery involves the removal of the bony outgrowth (exostosis) and the realignment of the bones of the joint. Soft tissue structures such as the ligaments and tendons may be repositioned and the bursa may be removed. The insertion of screws and pins may be required to stabilise the bones in their new, realigned position. Overview
If your teen or preteen is complaining of heel pain, it might be Sever?s disease. No need to stress - this isn?t actually a ?disease,? but rather a common type of growing pain that only lasts a few weeks or months and doesn?t leave any long-term damage. Sever?s disease occurs in kids as they hit their adolescent growth spurt, usually between the ages of 8-13 for girls and 10-15 for boys. It?s most common among active kids that run, play basketball or soccer, or do gymnastics. Kids with flat feet, high arches, short leg syndrome, over-pronation (feet that roll inward when they walk) or who are overweight or obese also have an increased risk. Causes The usual cause is directly related to overuse of the bone and tendons in the heel. This can come from playing sports or anything that involves a lot of heel movement. It can be associated with starting a new sport, or the start of a new season, or too much weight bearing on the heel. Also, excessive traction could cause this, since the bones and tendons are still developing. Many children who over pronate their feet exhibit symptoms and in most patients, it usually involves both heels. Symptoms Activity-related pain that occurs on the back of the heel, where the Achilles tendon attaches on to the heel bone. Tenderness, pain & swelling on the heel bone. Difficulty walking or walking with a limp or on tiptoes. Diagnosis In Sever's disease, heel pain can be in one or both heels. It usually starts after a child begins a new sports season or a new sport. Your child may walk with a limp. The pain may increase when he or she runs or jumps. He or she may have a tendency to tiptoe. Your child's heel may hurt if you squeeze both sides toward the very back. This is called the squeeze test. Your doctor may also find that your child's heel tendons have become tight. Non Surgical Treatment The treatment of Sever's disease should be individualized. The most important first steps in the treatment of Sever's disease are activity modification (including rest and sometimes crutches) and good shoes. Further treatment may include icing to decrease pain around the calcaneal apophysis, stretching and strengthening exercises, shoe orthotics or medications to relieve pain. Rarely, a removable cast is necessary to completely rest the foot.
Overview
 Achilles Tendon Rupture Surgery is a surgical procedure is used to repair a ruptured Achilles tendon. There are two types of surgery an open surgery and a percutaneous surgery, in both cases the surgeon sews the tendon back together through the incision helping the tendon to heal properly and restore function to the foot and ankle. If the injury or rupture has caused severe swelling the surgery may be delayed for a short period of time to allow the swelling to go down. Achilles Tendon Rupture Surgery is a surgical procedure is used to repair a ruptured Achilles tendon. There are two types of surgery an open surgery and a percutaneous surgery, in both cases the surgeon sews the tendon back together through the incision helping the tendon to heal properly and restore function to the foot and ankle. If the injury or rupture has caused severe swelling the surgery may be delayed for a short period of time to allow the swelling to go down.Causes Often the individual will feel or hear a pop or a snap when the injury occurs. There is immediate swelling and severe pain in the back of the heel, below the calf where it ruptures. Pain is usually severe enough that it is difficult or impossible to walk or take a step. The individual will not be able to push off or go on their toes. Symptoms Many people say that a ruptured Achilles feels like ?being shot in the heel?, if you can imagine how enjoyable that feels. You may hear a snap sound or feel a sudden sharp pain when the tendon tears. After a few moments, the pain settles and the back of the lower leg aches. You can walk and bear weight, but you may find it difficult to point the foot downward or push off the ground on the affected side. You will be unable to stand on tiptoe. Bruising and swelling are likely, and persistent pain will be present. Similar symptoms may be caused by an inflamed Achilles tendon (Achilles tendonitis), a torn calf muscle, arthritis of the ankle, or deep vein thrombosis in the calf, so an MRI or ultrasound scan will likely be used to diagnose your condition. Diagnosis During the physical exam, your doctor will inspect your lower leg for tenderness and swelling. In many cases, doctors can feel a gap in your tendon if it has ruptured completely. The doctor may also ask you to kneel on a chair or lie on your stomach with your feet hanging over the end of the exam table. He or she may then squeeze your calf muscle to see if your foot will automatically flex. If it doesn't, you probably have ruptured your Achilles tendon. If there's a question about the extent of your Achilles tendon injury, whether it's completely or only partially ruptured, your doctor may order an ultrasound or MRI scan. These painless procedures create images of the tissues of your body. Non Surgical Treatment The best treatment for a ruptured Achilles tendon often depends on your age, activity level and the severity of your injury. In general, younger and more active people often choose surgery to repair a completely ruptured Achilles tendon while older people are more likely to opt for nonsurgical treatment. Recent studies, however, have shown fairly equal effectiveness of both operative and nonoperative management. Nonsurgical treatment. This approach typically involves wearing a cast or walking boot with wedges to elevate your heel; this allows the ends of your torn tendon to heal. This method can be effective, and it avoids the risks, such as infection, associated with surgery. However, the likelihood of re-rupture may be higher with a nonsurgical approach, and recovery can take longer. If re-rupture occurs, surgical repair may be more difficult.  Surgical Treatment Operative treatment involves a 6cm incision along the inner side of the tendon. The torn ends are then strongly stitched together with the correct tension. After the operation a below knee half cast is applied for 2 weeks. At 2 weeks a brace will be applied that will allow you to move the foot and fully weight-bear for a further 6 weeks. After this you will need physiotherapy. Surgery carries the general risks of any operation but the risk of re-rupture is greatly reduced to 2%. The best form of treatment is controversial with good results being obtained by both methods but surgery is generally recommended for patients under 60 years of age who are fit and active with an intra-substance tear. Prevention To reduce your chance of developing Achilles tendon problems, follow the following tips. Stretch and strengthen calf muscles. Stretch your calf to the point at which you feel a noticeable pull but not pain. Don't bounce during a stretch. Calf-strengthening exercises can also help the muscle and tendon absorb more force and prevent injury. Vary your exercises. Alternate high-impact sports, such as running, with low-impact sports, such as walking, biking or swimming. Avoid activities that place excessive stress on your Achilles tendons, such as hill running and jumping activities. Choose running surfaces carefully. Avoid or limit running on hard or slippery surfaces. Dress properly for cold-weather training and wear well-fitting athletic shoes with proper cushioning in the heels. Increase training intensity slowly. Achilles tendon injuries commonly occur after abruptly increasing training intensity. Increase the distance, duration and frequency of your training by no more than 10 percent each week. Overview
Neuromuscular. Muscle imbalance causing different pull on pelvis (anterior superior Ilium or posterior inferior ilium). Muscle tightness/shortness especially piriformis (which lead to an external rotation of the femur thus shortening of the leg) and QL (raising ipsilateral iliac crest). Genu recurvatum, valgus, varus. Asymmetrical fallen arches or over pronation. Polio, Cerebral palsy. Trauma. Fracture. Injury epiphyseal plate. Iatrogenic (such as hip or knee surgery). Idiopathic. Hip disorder (such Legg-Perthes-Calve? or Slipped capital femoral epiphysis). Advanced degenerative changes. 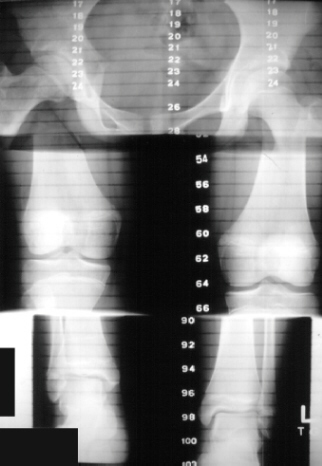 Causes LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio. Symptoms The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result. Diagnosis The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used. Non Surgical Treatment Heel lifts Raise the heel on the shorter leg. It is applied either to the heel of the custom orthotic or to the inside of the shoe under the insole at the heel. Generally if the discrepancy is greater than 3/8 of an inch, the modification is applied externally on the footwear. Custom made orthotics help to provide proper support and alignment to the foot, controlling conditions such as over pronation. Orthopedic Footwear, properly fitted, to which a lift might be applied inside or out.  Surgical Treatment In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
Overview
Adult acquired flatfoot deformity (AAFD) is a painful condition resulting from the collapse of the longitudinal (lengthwise) arch of the foot. As the name suggests, this condition is not present at birth or during childhood. It occurs after the skeleton is fully matured. In the past it was referred to a posterior tibial tendon dysfunction (or insufficiency). But the name was changed because the condition really describes a wide range of flatfoot deformities. AAFD is most often seen in women between the ages of 40 and 60. This guide will help you understand how the problem develops, how doctors diagnose the condition, what treatment options are available.  Causes Overuse of the posterior tibial tendon is often the cause of PTTD. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking, or climbing stairs. Symptoms Patients often experience pain and/or deformity at the ankle or hindfoot. When the posterior tibial tendon does not work properly, a number of changes can occur to the foot and ankle. In the earlier stages, symptoms often include pain and tenderness along the posterior tibial tendon behind the inside of the ankle. As the tendon progressively fails, deformity of the foot and ankle may occur. This deformity can include progressive flattening of the arch, shifting of the heel so that it no longer is aligned underneath the rest of the leg, rotation and deformity of the forefoot, tightening of the heel cord, development of arthritis, and deformity of the ankle joint. At certain stages of this disorder, pain may shift from the inside to the outside aspect of the ankle as the heel shifts outward and structures are pinched laterally. Diagnosis Posterior Tibial Tendon Dysfunction is diagnosed with careful clinical observation of the patient?s gait (walking), range of motion testing for the foot and ankle joints, and diagnostic imaging. People with flatfoot deformity walk with the heel angled outward, also called over-pronation. Although it is normal for the arch to impact the ground for shock absorption, people with PTTD have an arch that fully collapses to the ground and does not reform an arch during the entire gait period. After evaluating the ambulation pattern, the foot and ankle range of motion should be tested. Usually the affected foot will have decreased motion to the ankle joint and the hindfoot. Muscle strength may also be weaker as well. An easy test to perform for PTTD is the single heel raise where the patient is asked to raise up on the ball of his or her effected foot. A normal foot type can lift up on the toes without pain and the heel will invert slightly once the person has fully raised the heel up during the test. In early phases of PTTD the patient may be able to lift up the heel but the heel will not invert. An elongated or torn posterior tibial tendon, which is a mid to late finding of PTTD, will prohibit the patient from fully rising up on the heel and will cause intense pain to the arch. Finally diagnostic imaging, although used alone cannot diagnose PTTD, can provide additional information for an accurate diagnosis of flatfoot deformity. Xrays of the foot can show the practitioner important angular relationships of the hindfoot and forefoot which help diagnose flatfoot deformity. Most of the time, an MRI is not needed to diagnose PTTD but is a tool that should be considered in advanced cases of flatfoot deformity. If a partial tear of the posterior tibial tendon is of concern, then an MRI can show the anatomic location of the tear and the extensiveness of the injury. Non surgical Treatment Nonoperative therapy for adult-acquired flatfoot is a reasonable treatment option that is likely to be beneficial for most patients. In this article, we describe the results of a retrospective cohort study that focused on nonoperative measures, including bracing, physical therapy, and anti-inflammatory medications, used to treat adult-acquired flatfoot in 64 consecutive patients. The results revealed the incidence of successful nonsurgical treatment to be 87.5% (56 of 64 patients), over the 27-month observation period. Overall, 78.12% of the patients with adult-acquired flatfoot were obese (body mass index [BMI] = 30), and 62.5% of the patients who failed nonsurgical therapy were obese; however, logistic regression failed to show that BMI was statistically significantly associated with the outcome of treatment. The use of any form of bracing was statistically significantly associated with successful nonsurgical treatment (fully adjusted OR = 19.8621, 95% CI 1.8774 to 210.134), whereas the presence of a split-tear of the tibialis posterior on magnetic resonance image scans was statistically significantly associated with failed nonsurgical treatment (fully adjusted OR = 0.016, 95% CI 0.0011 to 0.2347). The results of this investigation indicate that a systematic nonsurgical treatment approach to the treatment of the adult-acquired flatfoot deformity can be successful in most cases.  Surgical Treatment In cases of PTTD that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required. For some advanced cases, surgery may be the only option. Surgical treatment may include repairing the tendon, tendon transfers, realigning the bones of the foot, joint fusions, or both. Dr. Piccarelli will determine the best approach for your specific case. A variety of surgical techniques is available to correct flexible flatfoot. Your case may require one procedure or a combination of procedures. All of these surgical techniques are aimed at relieving the symptoms and improving foot function. Among these procedures are tendon transfers or tendon lengthening procedures, realignment of one or more bones, or insertion of implant devices. Whether you have flexible flatfoot or PTTD, to select the procedure or combination of procedures for your particular case, Dr. Piccarelli will take into consideration the extent of your deformity based on the x-ray findings, your age, your activity level, and other factors. The length of the recovery period will vary, depending on the procedure or procedures performed.
Overview
There are some things that gain value as they age. Antique dealers are always on the lookout for pieces that have a certain ?wear and tear? look that will bring a high price tag. Our feet on the other hand, don?t always fair as well when they have experienced a lot of wear and tear. Cumulative stress and impact can cause your foot structure to weaken and become prone to injury, especially when you have a flat foot. This is the case with a condition called posterior tibial tendon dysfunction.  Causes Women are affected by Adult Acquired Flatfoot four times more frequently than men. Adult Flatfoot generally occurs in middle to older age people. Most people who acquire the condition already have flat feet. One arch begins to flatten more, then pain and swelling develop on the inside of the ankle. This condition generally affects only one foot. It is unclear why women are affected more often than men. But factors that may increase your risk of Adult Flatfoot include diabetes, hypertension, and obesity. Symptoms Patients will usually describe their initial symptoms as "ankle pain", as the PT Tendon becomes painful around the inside of the ankle joint. The pain will become more intense as the foot flattens out, due to the continued stretching and tearing of the PT Tendon. As the arches continue to fall, and pronation increases, the heel bone (Calcaneus) tilts into a position where it pinches against the ankle bone (Fibula), causing pain on both the inside and outside of the ankle. As the foot spends increased time in a flattened, or deformed position, Arthritis can begin to affect the joints of the foot, causing additional pain. Diagnosis Starting from the knee down, check for any bowing of the tibia. A tibial varum will cause increased medial stress on the foot and ankle. This is essential to consider in surgical planning. Check the gastrocnemius muscle and Achilles complex via a straight and bent knee check for equinus. If the range of motion improves to at least neutral with bent knee testing of the Achilles complex, one may consider a gastrocnemius recession. If the Achilles complex is still tight with bent knee testing, an Achilles lengthening may be necessary. Check the posterior tibial muscle along its entire course. Palpate the muscle and observe the tendon for strength with a plantarflexion and inversion stress test. Check the flexor muscles for strength in order to see if an adequate transfer tendon is available. Check the anterior tibial tendon for size and strength. Non surgical Treatment Conservative (nonoperative) care is advised at first. A simple modification to your shoe may be all that???s needed. Sometimes purchasing shoes with a good arch support is sufficient. For other patients, an off-the-shelf (prefabricated) shoe insert works well. The orthotic is designed specifically to position your foot in good alignment. Like the shoe insert, the orthotic fits inside the shoe. These work well for mild deformity or symptoms. Over-the-counter pain relievers or antiinflammatory drugs such as ibuprofen may be helpful. If symptoms are very severe, a removable boot or cast may be used to rest, support, and stabilize the foot and ankle while still allowing function. Patients with longer duration of symptoms or greater deformity may need a customized brace. The brace provides support and limits ankle motion. After several months, the brace is replaced with a foot orthotic. A physical therapy program of exercise to stretch and strengthen the foot and leg muscles is important. The therapist will also show you how to improve motor control and proprioception (joint sense of position). These added features help prevent and reduce injuries.  Surgical Treatment For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems. |
